Impingement syndrome is a common shoulder condition seen in middle aged and aging adults. This condition is also related to shoulder bursitis and rotator cuff tendinitis or rotator cuff tea. These conditions may occur alone or in combination.
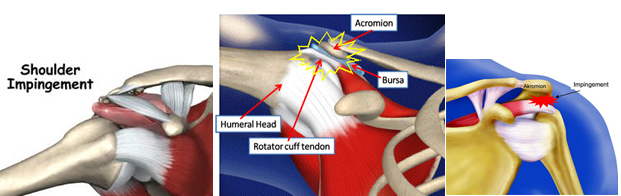
In most parts of the body, the bones are surrounded by muscles. In the shoulder region, however, the muscle is surrounded by bone. If one taps on the top of the shoulder, bone can be felt immediately under the skin. Underneath that bone is the muscle that lifts the arm. The rotator cuff muscles of the shoulder are sandwiched between the arm bone and the top of the shoulder (acromion). This unique arrangement of muscle between bone leads to the condition of impingement syndrome (shoulder bursitis, rotator cuff tendinitis).
When an injury to the rotator cuff muscle occurs, the muscle responds by swelling much the way an ankle does when it is sprained. However, because the rotator cuff muscle is surrounded by bone, its swelling causes a number of events to occur. The pressure within the muscle increases, resulting in compression and loss of blood flow in the small blood vessels called capillaries. When the blood flow is diminished, the muscle tissue begins to fray much like a rope. As the muscle tissue swells, it results in the classic features of a pain characterized like a toothache. Pain is aggravated by actions such as reaching up behind the back and reaching up overhead. Night pain resulting from this shoulder condition may result in sleep interruption.
The typical symptoms of shoulder impingement syndrome include difficulty reaching up behind the back, pain when the arms are extended above the head, and a weakness of shoulder muscles.If shoulder muscles are injured for a long period of time, the muscles can actually tear in two. The resulting injury is called a rotator cuff tear. This causes very significant weakness and, on occasion, inability to elevate the arm against gravity. Some patients will have rupture of their biceps muscle as part of this continuing impingement process.
Diagnosis begins with a medical history and physical examination. X-rays are helpful to rule out arthritis and will show changes in the bone that reflect the injury of the muscle. There may be bone spurs present or changes in the normal contour of the bone where the rotator cuff muscles normally attach. Impingement syndrome may be confirmed when an injection of a small amount of an anaesthetic into the space under the acromion relieves pain.
It is important to understand that the patient and the physician must treat the condition, not just the symptom. Oral anti-inflammatories, such as diclofenac, naproxen or piroxicam, remain the most common treatment of this condition. A patient must consistently take the medication for nearly 6 to 8 weeks to effectively treat the condition. Taking anti-inflammatories for a short period of time may treat the symptom of pain, but it will not treat the underlying problem. There is no specific medication for this condition and the effectiveness of any given medication varies by patient. If one oral medication is not found beneficial within 10 to 14 days, another oral anti-inflammatory drug may be used.
In addition to oral anti-inflammatory medications, daily stretching in a warm shower will help. Patients should work to reach a thumb up and behind the back. People with shoulder injuries should avoid repetitive activities with their injured arms, particularly activities in which the elbow would move above shoulder level. Activities which needs repeated overhead elevation of the arm needs to be avoided to minimize the use of the sore muscle.
If a patient has persistent symptoms despite the use of oral anti-inflammatories, a locally acting steroid injection may be considered by your doctor. Steroid is a potent anti-inflammatory drug that should be used only by specialist doctor, well experienced in giving this type of injections at the precise location where it is needed to be given, otherwise it can result in weakening of muscle tendon tissue. The mechanism of how this technique may be helpful is not completely clear, but it may reduce bursal and tendon irritation and swelling. The cortisone does not just "mask" the problem, but helps break the cycle of pain, swelling, weakness, and continued impingement. Injection therapy may then help reduce pain and impingement and allow the individual to continue to work on rotator cuff strengthening. Current recommendations are that a maximum of 3 cortisone injections should be used per shoulder. There is some evidence in laboratory research that more than 3 cortisone injections around an otherwise healthy tendon may result in considerable weakening of the tendon and even rupture.
If symptoms persist or if significant weakness is present (a possible symptom of rotator cuff muscle tear), your physician may perform an MRI scan. If the rotator cuff is torn, surgery may be necessary.
The vast majority of patients who have impingement syndrome are successfully treated with medication, stretching exercises, steroid injections, the temporary avoidance of repetitive overhead activity until the condition improves.